Skip to content
Call Now! 813-416-9531
wecare-healthcare
wecare-healthcare
wecare-healthcare
wecare-healthcare
wecare-healthcare
wecare-healthcare
wecare-healthcare
Welcome to WeCare Healthcare & Associates
wecare-healthcare
ENROLL IN FREE HEALTH INSURANCE
Apply Now
What We’re Offering
How It Works
1. Fill Out Form
2. Evaluation
3. Get Free Health Insurance
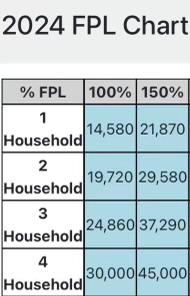
If you and your family income is in the purple range, you qualify to enroll year-round for a health plan. Apply Now!
Please enable JavaScript in your browser to complete this form.
Referred By:
*
Legal FIRST and LAST Name as it appears on you Social Security Card
*
First
Last
Date of Birth
*
Complete Social Security Number(To verify U.S. citizenship)
*
Gender
*
Male
Female
Race *
Physical Address
*
Street Address
*
Address Line 1
City
Alabama
Alaska
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Ohio
Oklahoma
Oregon
Pennsylvania
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
State
Zip Code
Mailing Address (If different from above)
Phone Number
*
Email
*
Marital Status
*
Single
Single
Married
If Married(Required) Complete the Section below: (Spouse Name,DOB, SSN)
Dependents as it appears on your 2022 tax return(Name,DOB,SSN):
Estimated Annual Income
*
Employer Name/Type of Work
*
Employer Phone Number
*
Upload Government ID and other Documents that’s required
*
Click or drag files to this area to upload.
You can upload up to 10 files.
Upload Other Documents such as Social Security Card & ETC
Click or drag files to this area to upload.
You can upload up to 10 files.
Would you be interested in receiving a phone call from our Agent to discuss dental and vision insurance options?
Yes
No
*Please read before signing.
By signing the box below, you attest that all of the information is true and correct to the best of your knowledge.
You are also giving licensed agents with WeCare Healthcare & Associates LLC, the permission to process your application with the information given.
I agree that if I am making less than $1500 per month that I am looking for work making at least minimum wage. I give the affiliate agent permission to access me and /my family marketplace account I agree this is a request to ENROLL in a FREE or next best available health plan. I agree if I already have a marketplace plan we may switch you to a better plan if one is available, if I am already on the best plan I am requesting the affiliate agent to become my agent of record from this point on unless notified in writing of the change. I agree to have my information used and retrieved from government data sources for this application. I have consent for all people I’ll list on the application for their information to be retrieved and used from government data sources. I understand that I’m required to provide true answers and that I may be asked to provide additional information, including proof of my eligibility for a Special Enrollment Period if I qualify. If I don’t, I may face penalties, including the risk of losing my eligibility for coverage. Renewal of coverage to make it easier to determine my eligibility for help paying for coverage in future years, I agree to allow the Marketplace to use my income data, including information from tax returns, for the next 5 years. The Marketplace will send me a notice, let me make any changes, and I can opt out at any time.
TAX ATTESTATION
I understand that I’m not eligible for a premium tax credit if I’m found eligible for other qualifying health coverage, like Medicaid, the Children’s Health Insurance Program (CHIP), or a job-based health plan. I also understand that if I become eligible for other qualifying health coverage, I must contact the Marketplace to end my Marketplace coverage and premium tax credit. If I don’t, the person who files taxes in my household may need to pay back my premium tax credit. I understand that because the premium tax credit will be paid on my behalf to reduce the cost of health coverage for myself and/or my dependents: I must file a federal income tax return for the 2023 tax year. I agree to FILE A FEDERAL INCOME Tax RETURN FOR THE 2023 TAX YEAR.
Disclosures and Disclaimers
*I grant WeCare Healthcare & Assocaiates LLC and/or its affiliates a limited power of attorney to help me get enrolled in the selected ACA Marketplace health insurance plan or an affordable Healthcare Plan. I also request that WeCare Healthcare & Assocaiates LLC use this limited power of attorney to automatically assist me in a plan for renewal on a annual basis* If Healthcare .gov require income verification or any other documents on my Marketplace application, I authorize WeCare Healthcare & Assocaiates LLC and it’s selective agents permission to submit those documents and a income verification estimation letter on my behalf using the estimated monthly/yearly income listed above.*
I agree that I am giving WeCare Healthcare & Assocaiates LLC and it’s Affiliates permission to collect my personal information, my ID, Social Security Card, Birth Certificate, Passport, Immigration form and other personal documents that may be required to assist me in enrolling in healthcare insurance through the Marketplace. *I also give WeCare Healthcare & Assocaiates LLC permission to send my information and my personal documents to healthcare agents and to the marketplace for free or affordable healthcare.
*I agree that after signing my electronic application through WeCare Healthcare & Assocaiates LLC and it’s affiliate’s. I give my permission to resubmit and copy and paste my signature on my behalf into the agents electronic portal/website to assist me in applying for healthcare insurance.
I’m signing this application under penalty of perjury, which means I’ve provided true answers to all of the questions to the best of my knowledge. I know I may be subject to penalties under federal law if I intentionally provide false information.
*I attest that all of the information below is true and correct to the best of my knowledge
Would you be interested in receiving a phone call from our Agent to discuss dental and vision insurance options? (copy)
Yes
No
Signature
Clear Signature
By signing above
Submit